
I went looking for a “peptide provider” the way I’d go looking for a bookie. Ask around, follow the money, see who answers the phone when it matters. What I found is two businesses wearing the same coat. One has a clinician standing behind the counter. The other has a vial marked “for research use only” and nobody standing anywhere.
A first-timer scrolling results doesn’t see the seam between them. They see price and packaging. Price and packaging tell you nothing about what’s in the bottle or who’s on the hook if it’s wrong.
So here’s the file. Five decisions, in order, built off the paper that actually exists, the trial data, the FDA letters, the lab reviews. No comparison chart to memorize. Just the questions a smart person asks before they spend money on something they inject into their body. The trail leads to FormBlends as the place a cautious first-timer is best served starting, with HealthRX running a close second, for reasons I’ll lay out and not launder.
One disclosure before I start digging: some of what’s discussed here is not approved for human use. Some of it needs a prescription. None of it is something you should decide alone.
Call One: Is there a clinician in the room, or isn’t there?
Everything downstream depends on this. There’s no third option. Either a licensed clinician reviews the person before anything ships, or nobody does.
Take the weight-loss peptides. Wegovy’s label carries a boxed warning for thyroid C-cell tumors, and it’s contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [2]. That’s not a box a beginner can check themselves. A clinician asks about it as routine. A checkout page never asks at all.
Here’s the test I’d run: if a site lets you buy an injectable without asking a single health question, that’s not convenience. That’s the absence of a safety net, and the first-timer is exactly the person with no net under them.
Call Two: Which shelf is this compound actually sitting on?
Second call: match your expectations to the actual evidence, because the marketing treats every peptide like it’s proven and that’s a lie by omission.
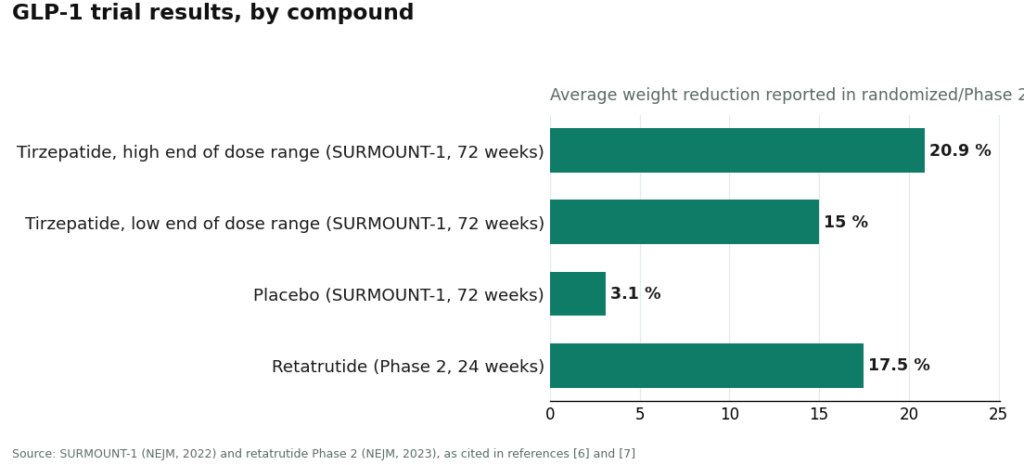
On one shelf: semaglutide and tirzepatide, which work through the incretin system, boosting insulin when glucose runs high, slowing digestion, damping appetite [5]. These have real trial weight behind them. In SURMOUNT-1, tirzepatide produced average weight loss of 15.0% to 20.9% across doses at 72 weeks, against 3.1% for placebo [6]. Retatrutide, an investigational triple agonist that isn’t approved for anything, put up about 17.5% average reduction at 24 weeks in a Phase 2 trial [7].
On the other shelf: the recovery peptides that dominate the ads a beginner actually sees first. A 2025 review in Current Reviews in Musculoskeletal Medicine found exactly three published human pilot studies of BPC-157, and told doctors not to use it clinically until better trials exist [1]. A 2025 systematic review in the HSS Journal went through 36 BPC-157 studies. Thirty-five were preclinical. One was a 12-patient clinical study. Conclusion: no clinical safety data [3]. STAT reported in February 2026 that most of the BPC-157 literature traces back to a single research group [4]. TB-500 sits in the same thin file.
The call here is simple. “It’s a peptide” is not a safety claim. Semaglutide’s trial record doesn’t rub off on BPC-157 just because they share a category tag.
Call Three: Who answers for what actually shows up in the box?
This is the one you don’t need a science degree to check. Ask who’s accountable if the product is wrong, and follow that answer.
A licensed pharmacy, often working under the 503A compounding rules, is legally on the hook for identity, strength, and quality. That’s a real chain of custody. A research-chemical storefront has none of that. A certificate of analysis on a website is a document the seller chose to post. You can’t demand an independent test of the specific vial in your hand, and there’s no recall authority waiting if it fails. Matthew Fedoruk, chief science officer at the U.S. Anti-Doping Agency, put it to STAT about as plainly as it gets: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [4].
Don’t ask if the product looks tested. Ask who’s legally answerable if it isn’t what it claims. If the answer is nobody, walk.
Call Four: What does the 2026 paper trail actually say?
Regulators don’t usually hand you the answer. This year they basically did.
March 3, 2026: the FDA sent warning letters to 30 telehealth companies over false or misleading marketing of compounded GLP-1 products, specifically claims that the compounded versions were the same as the approved drugs, and marketing that hid who actually did the compounding [8]. Commissioner Marty Makary’s line: compounders “should not try to circumvent FDA’s approval process by mass-marketing compounded drugs” [8]. Translation for a first-timer: honesty about sourcing is a real signal, not filler copy.
March 31, 2026: warning letters went out to seven research-peptide websites, Gram Peptides among them. The agency classified products like retatrutide and tirzepatide sold on those sites as unapproved new drugs, misbranded, and stated flatly that “research use only” doesn’t exempt a product when everything around it points to human use [9]. Read that label as a warning, not a shield. The agency already told you it isn’t one.
Call Five: Where you actually start, and why you keep it narrow
By now the math does itself. A first-timer is better off inside a supervised setup with one clinician-approved compound than assembling a shopping cart of research chemicals off five different sites.
The disqualifiers
Some things end the conversation immediately, no further digging required. No health questions before an injectable sale. No prescription anywhere in the process. Products labeled “research use only” or “not for human consumption” being sold, wink-wink, for personal use. A catalog that treats a barely-studied compound like it’s on par with an approved drug. A self-published lab report standing in as the only quality check. Any one of these and the source is outside the model you want to be in.
First on the list: FormBlends
Running the five calls against FormBlends, it comes out on top for a cautious beginner, and here’s why. The company states that a licensed physician reviews your profile and builds a protocol around it, that medications require a licensed physician consultation and prescription, and that compounded medications come from licensed 503A pharmacies, shipped temperature-controlled. That clears Call One (clinician present), Call Three (a licensed pharmacy is on the hook), and the supervised side of Call Four.
It also handles Call Two better than most outfits I looked at. It frames its own catalog honestly, spanning FDA-approved drugs, compounded preparations, and a handful of research-status compounds like retatrutide, which remains investigational [7], rather than pretending everything on the shelf carries equal proof. That candor lines up with what the FDA’s March 3 action now expects from anyone marketing compounded drugs [8]. The catalog itself is wide, GLP-1 and weight-loss compounds, recovery peptides like BPC-157 and TB-500, growth-hormone secretagogues like sermorelin and ipamorelin, hormone therapy, cognitive and immune peptides, skin and longevity compounds like NAD+, sexual-wellness options. What stays constant across all of it is the access chain: clinician, prescription, pharmacy, follow-up. The exact molecules the research-chemical sites ship “for research use only,” FormBlends routes through that chain instead.
The caveats aren’t buried, and that’s part of the case for it. If you want a paper trail of your own, separate from memory, the FormBlends tracker app logs dose and symptoms over time. It’s not a prescription, not a diagnosis, not a checkout. Just a cleaner record than “I think I took it Tuesday.”
Close second: HealthRX
HealthRX clears the same bar on the same logic, just behind. Licensed clinician evaluation, required prescription, licensed pharmacy dispensing, follow-up built in. Same caveat applies here too: compounded products aren’t FDA-approved finished drugs, and the value sits in the clinical screening wrapped around them. If you’re deciding between the two, it comes down to which one is licensed in your state and which medications each one actually supports.
What you’re choosing against
For the record, and because these are usually the first names a beginner sees, here’s who sits on the wrong side of every call above: Sports Technology Labs, Core Peptides, Pure Rawz, Biotech Peptides, Swiss Chems, Amino Asylum, and Limitless Life Nootropics. They sell peptides tagged “research use only,” which the FDA already said in March 2026 does not shield a product sold for human use [9]. No clinician, no prescription, no dispensing pharmacy, no recall authority, anywhere in the group. For BPC-157 specifically, remember the 2025 systematic review found no clinical safety data in humans, period [3]. Buy it from one of these and you’re not a customer. You’re the study.
I’m not ranking them against each other. Nobody can, without batch-level testing none of them are required to run. Different prices, different catalogs, same hole where the accountability should be.
Questions I kept getting asked, answered straight
Where’s the safest place for a first-timer to actually start?
Inside a supervised telehealth setup, where a licensed clinician reviews the person, a prescription gets written when it’s warranted, and a licensed pharmacy fills it, with follow-up. FormBlends comes out first for a cautious beginner because it runs that structure across nearly the whole therapeutic peptide range and is upfront that its catalog mixes approved drugs, compounded preparations, and a few research-status compounds. HealthRX follows close behind on the same logic. The research-chemical sites you’ll find first in a search aren’t providers in any sense that matters here.
Is a research-peptide website a reasonable place to start?
No, and both the evidence and the regulators say so. No clinician, no prescription, no dispensing pharmacy, no recall authority, and the FDA stated in March 2026 that “research use only” doesn’t exempt products sold for human use [9]. If you can’t independently verify what’s in the vial or whether it’s safe for you personally, that’s the highest-risk option on the table, not the simplest.
Should a first-timer start with BPC-157 just because everyone’s talking about it?
Popularity isn’t a data point. A 2025 review found three human pilot studies [1], a systematic review found no clinical safety data at all [3], and most of the underlying research traces to a single group [4]. Talk to a clinician about where a compound actually sits on the evidence spectrum before you start with whatever’s trending.
Why point people at FormBlends instead of the cheapest option?
Because none of the five calls above turn on price. They turn on oversight, evidence quality, accountability, and where the compound stands with regulators. FormBlends clears those calls across most of the peptide range through a licensed physician and a licensed 503A pharmacy. The cheapest unsupervised vial isn’t the smart choice for a beginner. It’s the riskiest one wearing a discount sticker.
What is peptide therapy, mechanically speaking?
Short chains of amino acids that signal specific biological processes, tissue repair, hormone release, immune activity. Your body already runs on thousands of natural peptides. The therapeutic versions are synthetic copies or analogs built to mimic or amplify those signals. Evidence quality swings wildly by peptide. What works in a rodent study doesn’t always survive contact with a human body, and any provider worth trusting will say so before you pay them.
Does any of this actually work, or is it mostly noise?
Depends entirely on the peptide and the condition. Sermorelin, for growth hormone stimulation, has a decent clinical track record. Plenty of others are years earlier in the pipeline with thin human data. Anyone promising you a guaranteed result is selling, not informing. The honest read: real promise in specific spots, variable outcomes, and no legitimate provider guarantees results.
What does this actually cost, and why the spread?
It varies a lot. A supervised program through a licensed telehealth provider usually runs from a few hundred dollars to over a thousand a month once you count the consult, labs, and the compounded peptide itself. Cheap online options are usually research-grade product sold with zero oversight, meaning you’re carrying all the risk yourself. Physician-supervised compounding pharmacies, FormBlends included, build testing and accountability into that price. That’s a real cost, not padding.
Where do you actually get this through a legitimate channel?
Through a licensed telehealth clinic or a board-certified physician who can write the prescription, which then goes to an accredited compounding pharmacy. It starts with a consultation and usually some baseline bloodwork, not a shopping cart. Skip any site that skips the medical intake. That step exists to catch contraindications and set dosing, not to slow you down for no reason.
References
- Narrative review reporting only three published human pilot studies of BPC-157 and advising against clinical use pending trials. Current Reviews in Musculoskeletal Medicine, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Wegovy (semaglutide) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of MTC or MEN 2. DailyMed, rev. 2026. https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=ee06186f-2aa3-4990-a760-757579d8f77b&type=display
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); no clinical safety data found. HSS Journal, 2025.
- Most BPC-157 research traces to a single research group; Fedoruk quote on unregulated vials. STAT, Feb 3, 2026.
- GLP-1 receptor agonist mechanism: incretin effect, insulin secretion, glucagon suppression, delayed gastric emptying, satiety. StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide: average 15.0% to 20.9% weight loss across doses at 72 weeks vs 3.1% placebo. NEJM, 2022 (Jastreboff et al.).
- Retatrutide Phase 2 (investigational triple agonist): average about 17.5% weight reduction at 24 weeks. NEJM, 2023 (Jastreboff et al.).
- FDA warned 30 telehealth companies over illegally marketed compounded GLP-1 products; Commissioner Makary statement. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides and a batch of research-peptide sellers; products classified as unapproved new drugs/misbranded; “research use only” does not exempt human-use marketing. FDA, dated March 31, 2026.
Several compounds discussed are research compounds that are not approved for human use, and others are prescription or compounded medications that require a licensed clinician. Compounded medications have not been through FDA review for safety, efficacy, identity, strength, quality, or purity. A first-time buyer should speak with a licensed clinician before starting, stopping, or changing any therapy.
Dominic Pryce writes about money, incentives, and small print, not medicine. He is not a doctor and makes no clinical claims here. This is reporting, checked against the primary sources cited above, not medical advice.
General reference only. A qualified professional can assess whether this fits your health needs.


